3 MARGINAL GAP
The performance of the luting materials and the chosen bonding technique have a decisive impact on the success of all-ceramic
restorations.
3.1.1 MATERIALS
Metal restorations rely principally on macroretention. By contrast
etchable all-ceramic materials (silicates/disilicates) are luted
directly to the hard dental tissues and rely on microretention. The
bond-ing of CEREC restorations (VITA Mark II, Ivoclar Empress CAD)
does not differ from the bonding of laboratory-fabricated inlays,
onlays and veneers made of comparable materials. This procedure
has remained virtually unchanged since the introduction of dentin
adhesives in 1991.
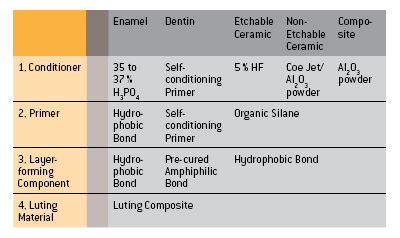
The first step is the CONDITIONING (e.g. etching) of the enamel,
dentin and ceramic with the goal of creating a clean micro-roughened
surface.
This is followed by the application of a PRIMER, the function of which
is to make the clean surface wettable for the hydrophobic bonding
material. The third logical step is BONDING – i.e. the application of
an unfilled bonding resin, which forms an intermediate layer
between the tooth surface, the luting composite and the ceramic
material.
Older adhesive systems consist of separate
products for each of
these steps. The newer systems try to reduce
the number of bottles
needed.
CONCLUSION The adhesive bonding of silicate ceramics has been proved
over a period of many years. The various materials must be
carefully matched.
High-strength oxide ceramics such as inCeram, aluminium oxide
and zirconium oxide do not lend themselves to etching and hence
can be conventionally cemented. Self-adhesive luting materials
have meanwhile become available.
Luting composites fall into three different categories: chemically
cured, light-cured and dual-cured.
This ten-year study compared CEREC 2 inlays which had been luted
either with chemically cured or dual-cured composites.
The success rate after ten years was 77% in the case of dual-cured
composite and 100% in the case of chemically cured composite.
CONCLUSION Dual-cured composites should be used only in situations
in which chemically cured or light-cured composites are
un-suitable.
3.1.2 MARGINAL SEAL
Shortly after the introduction of CEREC there were naturally no
long-term studies to draw upon. It was therefore necessary to establish
whether the width of the luting interface (i.e. the thickness
of the luting composite layer) had any influence on the marginal
seal.
All the investigations showed that it was advantageous to locate
the restoration margin in the enamel. This in vitro study (which
involved dye penetration tests) showed that the thickness of the
luting composite layer did not have any influence on the marginal
seal. Subsequent long-term studies of CEREC 1 and CEREC 2 restorations
confirmed these findings.
CONCLUSION The thickness of the luting composite layer does not have
any influence on the marginal seal.
In relation to deep cavities the question is whether a liner plays a
beneficial role for the protection of the pulp.
According to a study carried out by N. Krämer/Erlangen the
occurrence of initial hypersensitivity doubled in cases where
a liner was laid. The failure rate of ceramic inlays (in this case
Empress) trebled when a liner was deployed.
CONCLUSION The placement of liners under ceramic inlays/onlays is
contra-indicated.
3.1.3 WEAR OF THE ADHESIVE INTERFACE
Various Empress inlays placed using Variolink low (low viscosity)
and Tetric (high viscosity) were measured in order to determine
the wear of the luting composite in highly loaded areas.
After 8 years the mean interfacial width had increased from 176
μm to 207 μm.
The two different composites did not exhibit any significant statistical
differences.
CONCLUSION Low-viscosity and high-viscosity composites are suitablefor the placement of CEREC inlays and onlays.
 |
3.2 COMPARISON OF OTHER RESTORATION TYPES
Temporaries and methods of bonding labside and chairside produced ceramic inlays have a decisive influence on enamel defects and
the margin quality.
3.2.1 ENAMEL INTEGRITY
Inlay cavities treated with temporaries demonstrate, after simulated
temporary wear in a chewing simulator, a deterioration of the
enamel integrity. In particular in both oral and vestibular surfaces
cracks developed. By cavities treated immediately with chairside
produced ceramic inlays no such enamel defects arose.
CONCLUSION Chairside produced CEREC inlays offer the treated tooth
a reduced risk of enamel cracks, due to there being no
provisional.
3.2.2 MARGIN QUALITY
The analysis of bonding systems demonstrated that conventional
bonding is still superior to self-adhesive systems. Selective enamel
etching as used with CEREC inlays enhances the bond with the
hard tooth tissue and improves the quality of the enamel margin.
In contrast to the general assumption a broader adhesive gap does
not result in inferior margin quality.
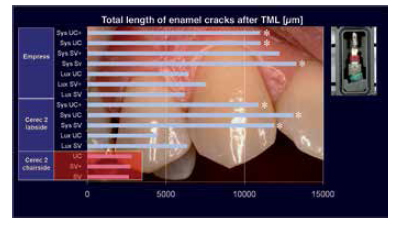
Measurement results of damage to the enamel marginal edge (with or without
temporaries). Chairside ceramic treated cavities show fewer enamel
cracks
[TML: thermocycling and mechanical loading].
|
CONCLUSION Immediate treatment without temporaries has a stabilizing
effect on the tooth substance. Attainable bonding technology
takes into account a broader adhesive gap.






