1 LONG-TERM PERFORMANCE
OF CEREC RESTORATIONS
1.1 INLAYS/ONLAYS
1.1.1 LONG-TERM STUDY OF 2,328 CHAIRSIDE INLAYS/ONLAYS
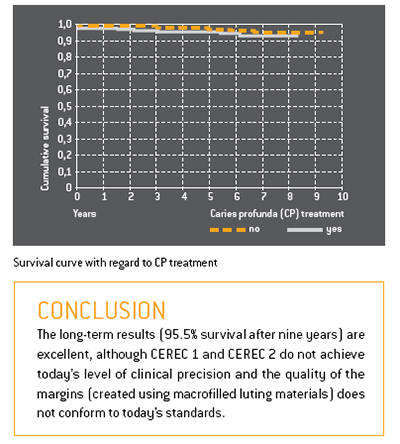
This extensive study centred on 2,328 chairside CEREC inlays and
onlays which had been fitted to a total of 794 patients in a dental
practice. Between 1990 and 1997 the CEREC 1 system had been
used; between 1997 and 1999 the CEREC 2 system was used.
Forty-four teeth were randomly selected and examined under
a scanning electron microscope. The average margin width was
236 μm ± 96,8 μm.
The success rate after nine years was 95.5%. Only 35 restorations
failed, due mainly to the extraction of the teeth. There was no correlation
between failure and the size or location of the restorations.
 |
1.1.2 EIGHTEEN-YEAR STUDY OF 1,011 INLAYS/ONLAYS
This study centred on 1,011 CEREC inlays/onlays which had been
fabricated for 299 patients between 1987 and 1990 using the
CEREC 1 system. The majority of the restorations were made of VITA
MK I ceramic; only a small number (22) were made of Dicor MGC. As from 1989 enamel etching (phosphoric acid) was deployed
in combination with the dental adhesive Gluma. Glass ionomer
cement
was no longer used as the base layer. Areas close to the
pulp were protected by means of a CaOH2 liner.
The follow-up criteria were as follows: margin quality, change in
vitality, tooth anatomy, complications, and failures.
The findings were categorized according to the following parameters:
restoration size, restoration location, initial tooth vitality, and
the use of dentin adhesive.
During the 18-year observation period 86 of the 1,011 restorations
were lost. Ceramic fractures were the main cause (38%).
According to the Kaplan Meier estimator, the probability of success
after 18 years was extremely high (84.4%). Premolars perform
slightly better than molars, and 2- and 3-surface inlays better than
1-surface inlays. There is a significance between non-vital teeth
(50%) and vital teeth (88%). The application of a functional dentin
adhesive increased the success rate by 10% to 90%.
1.2 VENEERS
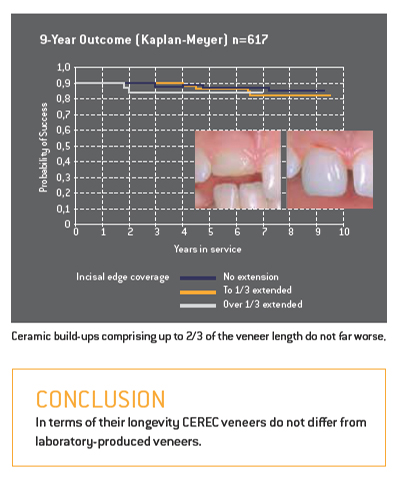
The durability of laboratory-produced ceramic veneers has already
been extensively researched. A group of CEREC veneers and partial
anterior crowns was observed over a period of 9.5 years. These restorations
had been produced on the CEREC 1 and CEREC 2 systems
using VITA Mark II (mainly) and Ivoclar ProCad. 509 of the veneers
had been bonded to natural teeth; 108 had been used to repair/
replace existing PFM or gold-composite restorations. After 9.5 years
the restorations attached to prosthetic elements had a success
rate of 91%, while those placed on natural teeth showed a success
rate of 94%.
 |
1.3 CROWNS
Following the introduction of CEREC 2 dentists were in a position to
produce full crowns in addition to inlays and veneers.
In a further scientific study 208 CEREC crowns made of VITA Mark II
were fitted to 136 patients using the adhesive bonding technique.
Seventy of these crowns were placed on conventionally prepared
teeth; 52 were placed on teeth with reduced stump preparations
(low macroretention); and 86 crowns were placed on endodontically
treated teeth. In this case the crowns included an additional
post extending into the pulp cavity in order to achieve improved
retention (endocrowns).
The main causes of failure were fractures, presumably due to inadequate
dentin adhesion.
The “classic” crowns performed best of all (97.0% survival rate),
followed by the “reduced” crowns (92.9%). The survival rate of the
endocrowns was acceptable in the case of molars (87.1%) and relatively
poor in the case of premolars (68.8%).
CEREC crowns also performed well in a study conducted in a dental
practice. This study centred on 65 full crowns made of VITA Mark II
which had been manually polished after the milling process and
then bonded using dual-curing composite.
Three failures were observed in the period up to four years (two
ceramic fractures, one debonding). The success rate according to
Kaplan-Meier was 95.4%.
CONCLUSION CEREC crowns made of VITA Mark II and Ivoclar ProCad achieve
success rates which are comparable to those PFM crowns.
1.4 COMPARISON WITH OTHER RESTORATION TYPES
1.4.1 CLINICAL COMPARISON
Long-term comparison of CEREC, laboratory-fabricated ceramic
and gold inlays over a period of 15 years.
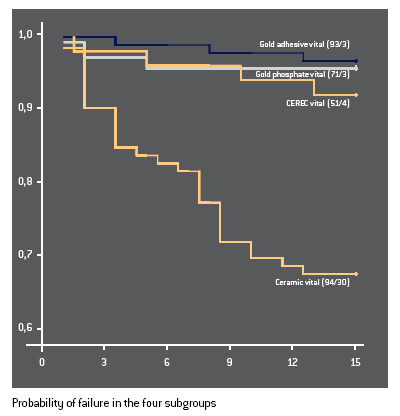
For the past 15 years 358 two- and three-surface inlays have
been under observation at Graz University in Austria. The following
restorations were placed on vital teeth: 93 gold inlays cemented
with zinc phosphate cement (= control group); 71 adhesively
bonded gold inlays; 94 laboratory-fabricated ceramic inlays
(Dicor, Optec, Duceram, Hi-Ceram); and 51 CEREC inlays (VITA
Mark I). In addition, a number of non-vital teeth were treated: gold/
cement (5); gold/adhesive (14); laboratory-fabricated ceramic
(22); and CEREC (8).
The restorations were assessed according to the following criteria:
loss or complete fracture; partial fracture of the restoration, the
tooth or the cement/adhesive bond; secondary caries; loss of tooth
vitality. A Kaplan-Meier survival analysis was carried out for each
group. In all groups inlays placed on non-vital teeth performed worse
than inlays placed on vital teeth.
Initially the study included a group of indirect composite inlays.
However, these were excluded prematurely on account of their very
poor performance.
There was no significant statistical difference between the gold
inlay groups and the CEREC inlays (success rate of approx. 93%
after 15 years). The laboratory-fabricated ceramic inlays were clearly
inferior (68%).
CONCLUSION In terms of longevity CEREC inlays are on a par with gold
restorations. The laboratory-fabricated ceramic restorations
performed worse.
The following ductile filling materials are used for posterior cavities:
amalgam; glass ionomer and derivative products; and composites.
In addition the following restoration types are available: gold inlays/
onlays; composite inlays/onlays; laboratory-fabricated ceramic
inlays/onlays; and CEREC inlays/onlays. Long-term studies have
been carried out for each group.
These have revealed significant differences in longevity. The annual
failure rate was determined for each restoration type. The ranking
(from bad to good) is as follows:
7. Glass ionomer and derivative products (7.7%)
6. Amalgam (3.3%)
5. Composite fillings (2.2%)
4. Composite inlays/onlays (2.0%)
3. Ceramic inlays/onlays (1.6%)
2. Gold inlays/onlays (1.2%)
1. CEREC inlays/onlays (1.1%)
CONCLUSION The success rates of CEREC restorations are marginally
better than those of gold inlays/onlays.
1.4.2 LONGEVITY AND COST-EFFECTIVENESS
In times of financial constraint it makes sense to evaluate the
longevity and cost of dental restorations – not in isolation but
in combination – in order to develop cost-effective restoration
options for patients.
On the basis of billing data provided by a major German insurer
the average fees and laboratory costs were determined for
gold inlays (62), laboratory-fabricated ceramic inlays (87) and
CEREC inlays (91). A meta analysis was then performed of ten
suitable long-term studies from the period 1994 to 2003. This
provided
the basis for determining the statistical longevity of the
various inlay types.
1.4.3 LONGEVITY AND PRODUCTION COSTS
Due to their higher production costs and slightly lower survival
probability, laboratory-fabricated ceramic inlays are the least
cost-effective option. Gold inlays and CEREC inlays have similar
success rates. However, given the higher laboratory costs of gold
inlays, CEREC inlays emerge from this study as the most costeffective
restoration
type.
Sources: Arnetzl
CONCLUSION From an economic viewpoint CEREC inlays are preferable to
all other inlay types.